Every year I dance the danger line, coming up with predictions for the upcoming year. And every year I hold myself accountable, reporting to you, loyal reader, exactly how those predictions worked out.
 Clearly not a self-portrait; I could never grow that facial hair…
Clearly not a self-portrait; I could never grow that facial hair…
So here’s this year’s results…
(predictions are here)
- Premiums will rise as employment and wages continue to grow.
It’s a yes. Rates continue to decline, but hourly wages have been ticking up for over a year now, and employment has been trending up for over 60 months. So, the combination has overcome the drop in rates. For now… - Medical costs will remain flat or close to it.
Not according to NCCI – at least not for last year in NCCI states. Medical costs increased 5 percent last year. California is not an NCCI state; trend was up 6 points last year. So, got that one wrong. - Frequency will continue to decline.
Because it always does. On average, by 3.6 percent a year.
That means there will be about 10 percent fewer claims in three years, 20% fewer in six. - Insurers will double down on efforts to reduce administrative expenses.
Frequency’s down, investment returns are dropping, and medical costs pretty much under control; premium rates are headed lower as well. So, insurers have continued their efforts to slash admin costs by outsourcing more claims to TPAs (contacts in the TPA business indicate that’s their biggest source of growth). - More payers will move their claims adjusters to home offices.
No news on this – so I’ll count this as a no. If you know of moves, let me know. - Winners will focus on execution.
Yes. MedRisk [HSA consulting client] has taken the top spot in physical medicine management from competitor OneCall by out-executing OC. PBMs that deliver seamless customer service, lower drug costs and reduced opioid spend are winning; myMatrixx is perhaps the best example. Kaiser Permanente on the Job is another example; K-PoJ is delivering better results for patients and employers by doing what KP does so well – focusing on what patients need, not what creates billing opportunities. And BWC Ohio has made amazing progress in reducing unnecessary opioid use – by developing and implementing a comprehensive, careful approach. - Telemedicine is coming fast
Yes indeed. Coventry, MedRisk (HSA consulting client), CHC Telehealth (Mitchell has helped fund CHC), Kura, and other entrants were all over the NWCDC. MedRisk’s telerehab program is up and running, and case management firms are moving quickly.
Unlike other “innovations”, tele-services is going to change everything.
8. Mitchell will continue to add work comp services businesses via acquisition.
Yes – Unimed and PMOA are additions this year, adding breadth to both the UR and PBM businesses. I’d expect more in the future – although there are fewer businesses to buy that fit well with the company’s strategy.
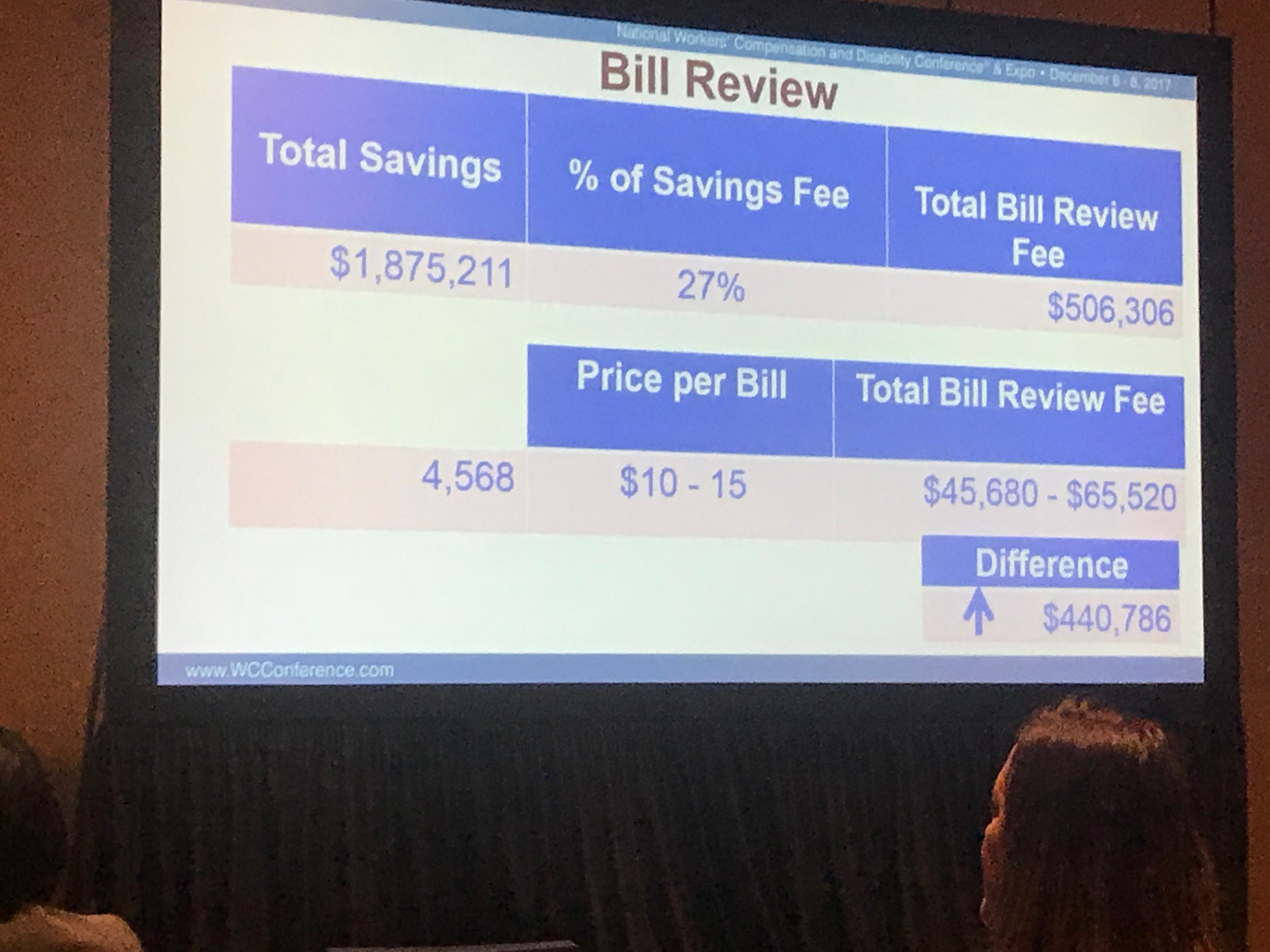
9. Drug cost decreases will flatten out somewhat, while reductions in opioid spend will continue to increase.
Well, I got this one partially – but pretty badly – wrong. Costs dropped by double digits, led by a 13.6 percent decline in opioids. And I’m supposed to know a lot about this business…sheesh.
10. More value-based payment pilots will hit work comp.
That’s a really easy prediction, so I’ll quantify it – there will be more than five new pilots or program seeking to deliver care via bundled payments or similar mechanisms that will start in 2017.
Well, except for K-PoJ I can’t find any evidence that this happened – and in fact in a post a few months after my 2017 predictions, I backtracked bigtime on this prediction. Any new news on this is welcomed.
11. Bonus pick – more consolidation in case management
As frequency and severity continue to slide, field case management businesses are going to have to find new revenues from new services they can offer to current clients/cases and get more revenue from current cases.
Argh…haven’t seen much evidence of this – perhaps because there’s already been a lot of consolidation.
The net – I got 4.5 wrong out of 11. Ouch.
I’m hoping to do a LOT better with next year’s prognostications.