This is way worse than we thought even a week ago. The death rate remains much higher than the flu, while we continue to get confusing and contradictory messages from the White House.
Facts.
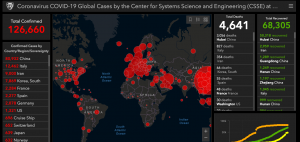
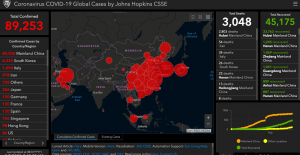
- In the US, the number of diagnoses has tripled over three days.
- The death rate is just shy of 2 percent – about 20 times greater than the regular flu.
- Italy remains the worst-affected country, with almost 25,000 confirmed cases and 1800 deaths – a death rate of 7.2 percent.
- Contrary to what you may have heard, Italy’s population is NOT the oldest in Europe – Germany’s people are slightly older – and many other countries are almost as old as Italy.

What will protect us?
Not this…
- face masks. those regular face masks are useless. Unless the facemask is specifically designed to eliminate most airborne moisture – and you have been trained specifically in how to fit the mask – it won’t protect you.
- Unless you are already ill – in which case those regular masks help limit others’ exposure.
- A vaccine. There will NOT BE A VACCINE for at least a year.
- Drugs – THERE ARE NO MEDICATIONS TO TREAT COVID-19.
This.
Wash your hands. Use alcohol-infused wipes.
Stay home.
Avoid any close contact with anyone you do not KNOW.
Sorry, grandma…I didn’t mean to kill you. For anyone younger than 30 or older than 60 reading this – forgive me for generalizing, but please stop doing stupid stuff. Going to St Patrick’s Day events, senior dance parties, concerts, beach parties, and bars won’t hurt you much (unless you are diabetic, asthmatic, have pulmonary issues, are obese, or have an immune deficiency (which you may find out the hard way) – but it will kill others who get Covid-19 from you.
Finally, what’s with this obsession with toilet paper?
If this is the beginning of the zombie apocalypse – which it most definitely is not – I’m thinking we should be ensuring there’s enough nutrition to go into our bodies – if there isn’t, we will not have to worry about taking care of what exits our bodies.
Okay, after ten days of nothing but Covid-19 blog posts, we’re going back to our regularly-scheduled focus on healthcare, healthcare policy, and workers’ comp stuff.