Several commenters purporting to be chronic pain patients responded to my post about the AMA’s bemoaning CDC’s opioid guidelines.
Their stories were tragic; heartfelt; full of pain, suffering, and grief. All decried the CDC’s guidelines as wildly misplaced, directly responsible for their terrible suffering, a governmental overreach, and a grossly misplaced intrusion of the government into the hallowed doctor-patient relationship.
Several attacked Dr Andrew Kolodny, making all kinds of ugly claims, attacking his ethics and denigrating his motivations. [Dr Kolodny is Executive Director of Physicians for Responsible Opioid Prescribing.]
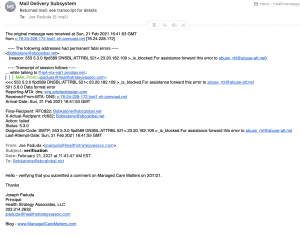
And all but one came from email addresses that are bogus. I know that because I emailed each of them and asked them to confirm they sent a comment to MCM. Here’s an example of one response.
I’ve known Dr Kolodny for over a decade. We met at the first few RxSummit conferences where colleagues introduced us. He was one of the first clinicians to raise the alarm about prescription opioids, and PROP has been instrumental in helping states, the CDC, and other governmental entities address the opioid crisis. I deeply respect Dr Kolodny – his relentless effort to stop the devastation caused by opioids has saved countless lives.
I do not know who is behind these attacks on the CDC and the attempts to libel and slander Dr Kolodny. I do not know if they are the product of the Opioid Industry, another example of their insidious effort to legitimize its criminal behavior and its lethal consequences. The Opioid Industry’s tentacles take the form of organizations that sound legitimate but are just mouthpieces for Big Opioids.
Big Opioid sponsors so-called patient advocacy groups, yet another example of Astroturfing (go to p 29, about halfway down, to see a description of the practice; or just search for Astroturf).
I also wrote on this several years ago.
The Astroturfers’ clever messaging convinces some chronic pain sufferers that the solution is more opioids, and anyone who disagrees is a self-serving, uncaring profiteer who is somehow profiting from their pain.
I hate Big Opioid and the people who propagate their lies. They are killing people, devastating families and destroying communities, all in the name of profits.
They are mass murderers – nothing less.