There’s a good deal of confusion out there about “natural” immunity and COVID.
Here are the facts.
first, there’s no such thing as “artificial” immunity. ALL immunity is natural…whether one is infected by COVID or gets a vaccination, the body has a natural response.
Virologist Stuart Neil:
all a vaccine does is prime the immune system with a dead pathogen, a protein (or part of a protein from it), or a related but harmless pathogen so that the body can respond so much more quickly when the actual pathogen is actually encountered…
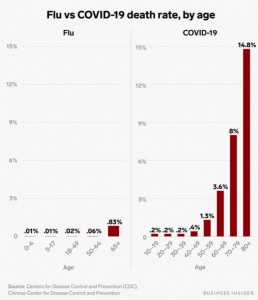
second, if you want to protect against a COVID infection, would you rather:
a) get a vaccine that is FDA approved, has been proven safe and effective, or:
b) get infected with COVID.
Sure, there can be side effects from COVID vaccines (a family member had a pretty nasty albeit brief headache and chill episode after his/her second Moderna jab, but I had no side effects from any of my three Pfizer shots). Balance that against the potentially much worse illness – or death – from a real COVID infection, and the choice is pretty obvious.
third, multiple recent studies prove that previous COVID infections are NOT as effective at preventing future COVID infections as are vaccines. Summary findings from two:
This study “found that the chances of these adults testing positive for COVID-19 were 5.49 times higher in unvaccinated people who had COVID-19 in the past than they were for those who had been vaccinated for COVID and had not had an infection before.”
And this one “indicates that if you had COVID-19 before and are not vaccinated, your risk of getting re-infected is more than two times higher than for those who got vaccinated after having COVID-19.”
Finally, if you were unlucky enough to have contracted COVID AND smart enough to get fully vaccinated, you’re even less likely to get COVID again.
Sure, there’s a LOT of misinformation out there, including this total distortion/misstatement/nonsense (just one – it was conducted BEFORE “most persons had received additional or booster COVID-19 vaccine doses to protect against waning immunity. (Actual study is here.)
But hey, if you want to fight science, go right ahead. Just remember what happened to Wile E Coyote when he denied gravity’s existence…

Oh, and if you do fall off the cliff, don’t get upset if healthcare workers are less than sympathetic.
What does this mean for you?
Get vaccinated. Wear a mask.
and a hat tip to Bill F for alerting me to the issue!



 Why?
Why?