Did exactly what it was intended to do – engaged with a lot of people, bluntly stating what many are thinking.
Some of the willingly unvaccinated are very good friends, people I admire, respect, and care about. It grieves me to no end that we are so far apart on this issue, and that it has come to this.
The title and some of the language offended a few (out of 2567 subscribers, 21 unsubscribed). While I absolutely do not apologize for my language I do understand why you may have been offended. Long time readers know that I almost never curse on MCM (although I am more profane in person); I think I’ve used profanity fewer than 5 times in over 3500 posts.
On the other side, 8 new subscribers signed up and comments and private emails were overwhelmingly supportive.
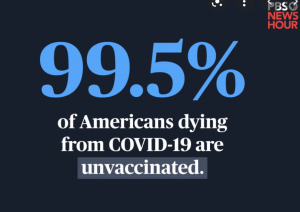
What is apparent is this. Anger with the willfully unvaccinated is growing, and for very good reason. Unless you are a Native or Black American or have a legitimate medical issue, you have no valid reason to put your family and friends and the rest of us at risk because you don’t want to get the vaccine.
(Native and Black Americans should absolutely get vaccinated; however knowing how we killed millions of Native Americans and infected Blacks in the name of science one can certainly understand vaccine fears, fears we must overcome.)
You have already been vaccinated to protect you from polio, mumps, measles, rubella, and many other childhood ailments. Many of us have vaccinations protecting us from the flu, tetanus, rabies, shingles and myriad other diseases.
You didn’t rebel, protest, or demonstrate when your kids had to get those vaccinations to attend school.
You didn’t scream and shout when you asked for a shingles vaccine to protect you from this painful and debilitating infection.
No one was outraged when we effectively ended small pox and polio infections through mass vaccinations.
So ask yourself – why are you so angry about COVID vaccines? And be honest. Do not spout meaningless nonsense you read somewhere on Facebook about VAERS or breakthrough infection issues or other blather. We are done refuting arguments that don’t stand up to the most cursory examination.
And I will publicly call out commenters who spout such idiocy.
The reason is tribalism. You and your friends and family have been duped into making COVID a divisive issue, to separate us and push us apart. After 20 months of attempting to educate, inform, discuss and debate, the majority of Americans are fed up with your intransigence, your willful ignorance, your refusal to accept the science.
I have tried and tried and tried again, writing over 120 posts about COVID only to be met with the same tissue-thin arguments based on nothing but a Facebook post.
So, we are done with you.
If you refuse to get vaccinated, then you get to own the consequences of your decision. You tout personal responsibility, you teach your kids to be responsible, you demand it of your elected officials, then fine – you get to:
- lose your job,
- pay for all your COVID-related medical care, and
- be sued for the care of others you infect.
What does this mean for you?
Your decisions have consequences. Own them.