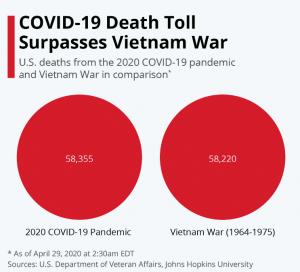
As of this morning 23,459 US deaths have been attributed to COVID19.
That number is almost certainly too low.
The words “have been attributed” were carefully chosen – note I did NOT write “COVID19 killed 23,459 people” or “23,459 people died of COVID19 or “there were 23,459 COVID19 deaths.”
Briefly, that’s because:
a) patients presenting at a hospital with breathing problems, a fever, and a bad headache are often not tested as COVID19 is assumed;
b) severe COVID cases typically lead to heart attack, Acute or Severe Respiratory Distress Syndrome or other problems, and the cause of death [more on this below] may be attributed to a heart attack/ARDS/SRDS and not to COVID;
c) many hospitalized victims also have other health problems; diabetes, high blood pressure, asthma, COPD, cardiac issues. These co-morbidities greatly increase the risk of death and, absent a positive test for COVID19, may be given as the cause of death; and
d) cause of death (COD) can be a judgment call, and multiple CODs can be reported on the “death certificate”.
Here are the facts.
The CDC finally published guidelines for assigning cause of death for COVID19 earlier this month. Needless to say, a lot of people had died from COVID19 before these guidelines came out, so that’s issue One; Issue Two – as noted above, there can be multiple “causes of death”.
For physicians confronted with a deceased patient, determining and assigning a cause or causes of death is often complicated and uncertain. For example, COVID19 leads to much greater stress on the heart as it tries to pump more blood to get more oxygen out of damaged lungs. According to the CDC, when that old, tired, sick heart gives out:
The immediate cause of death [in this case the heart attack], which is the disease or condition that directly preceded death and is not necessarily the underlying cause of death (UCOD) [in this case COVID19], should be reported on line a. The conditions that led to the immediate cause of death should be reported in a logical sequence in terms of time and etiology below it [on the cause of death statement]. [italics added]
Last week, CDC spokesman Scott Pauley said, “It’s likely that COVID-19 related deaths may not be included on a death certificate [italics added] or COVID-19 might be a factor related to an individual’s death but not the main cause.”
Issue Three – no test, no diagnosis (in some cases) From ABCNews last week
“There is no swabbing of deceased individuals anymore and unless the medical examiner has knowledge of a confirmed coronavirus test, then they aren’t being marked down as having coronavirus,” said [New York City Councilman Mark] Levine, whose committee has oversight for the Office of the Chief Medical Examiner.
Issue Four – A related issue is most of the victims of COVID19 are elderly; older people who contract COVID19 are much more likely to die than younger folk.
Of course, older people have more health problems than younger folks, so there are more “potential” causes of death – cancer, heart disease, stroke, hypertension, COPD, kidney failure and the like. Thus there are more opportunities for the pathologist to attribute non-COVID causes as one of the causes of death – which would further skew the numbers.
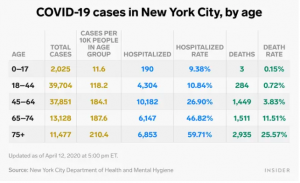
There are compelling data from New York City indicating COVID19 may be involved in many more deaths than have been attributed to the virus;
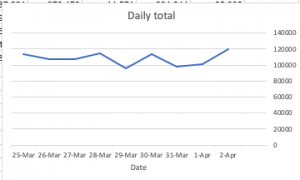
The FDNY reported a nearly 400 percent increase in “cardiac arrest” home deaths in late March and early April, [emphasis added] a spike that officials say is almost certainly driven by COVID-19, whether they were formally diagnosed or not.
Between March 20 and April 5, the department recorded nearly 2,200 such deaths, versus 450 in the same period last year,
Then there’s the issue (Five, to those still counting) that there are a LOT of “extra” deaths that can’t be directly tied to COVID19 as that specific cause of death, however these “extra deaths” happened during the COVID19 crisis.
This from Judy Melinek M.D., a forensic pathologist:
To quote Dr. Ed Donoghue, a forensic pathology colleague at the Georgia Bureau of Investigation, “No matter how these deaths are currently being attributed, after this pandemic terminates, an excellent approximation of the true fatality rate of COVID-19 deaths can be made by the calculation of the excess mortality for the period. This calculation was very helpful during the 1995 Chicago heat wave. Almost certainly, because of the scarcity of testing and other reasons, we will find that the number of COVID-19 deaths has been grossly underestimated.”
Okay, counterclaims. There are any number of specious claims about rampant over-counting of deaths as COVID; I have yet to see any from any credible source backed by credible data. This is perhaps the best overall discussion of claims that COVID deaths are overcounted; it is thorough and detailed.
Here are just a couple debunked claims…
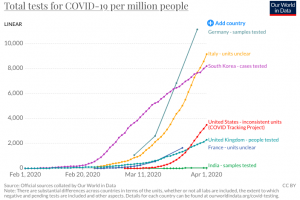
For those interested – The international picture
From the BBC – “it might seem simple enough: if a patient dies while infected with Covid-19, they died of Covid-19.” Perhaps – but they may have died from a car accident, or might have an underlying health condition such as COPD or asthma or heart disease. The UK counts ANYONE who dies and has tested positive for COVID as a COVID death. Even if they died in a car accident.
A related issue – reports from Italy indicate there are a lot more people dying of all causes than usual, and many of those “extra” deaths aren’t attributed to COVID. “Only 12 per cent of death certificates have shown a direct causality from coronavirus,” said the scientific adviser to Italy’s minister of health last week. [source here]
What does this mean for you?
Two things:
We do not KNOW how many deaths are directly or indirectly due to COVID19. But medical experts, physicians, epidemiologists, and medical examiners believe it is significantly higher than the published total.
There are truckloads of BS on the interwebs about COVID; ignore anything not based on solid research from credible people with scientific and/or clinical training and experience.