Holy bejeezus this has been a crazy week.
Labor Secretary Nominee
First up, the nominee for Labor Secretary is fast food executive and avowed billionaire Adam Puzder. Puzder’s likely to face tough questioning from Democrats for his stance on the minimum wage, automation, mandatory sick leave, and ACA. He’s also been a vocal critic of the overtime rule.
His restaurants paid a $9 million fine re class action lawsuits involving overtime pay in 2004.
For those in the workers’ comp world concerned about a new Commission on work comp, your concerns are gone.
Puzder’s points on automation aren’t crazy – in point of fact there’s a lot of research on the impact of automation on jobs, with one very credible group estimating 47% of jobs will be automated within 25 years.
Drug prices
Adam Fein has an excellent post on drug pricing, diving into the list v actual price. Adam uses the EpiPen and insulin products as examples. For those involved in pharma, this is a must read.
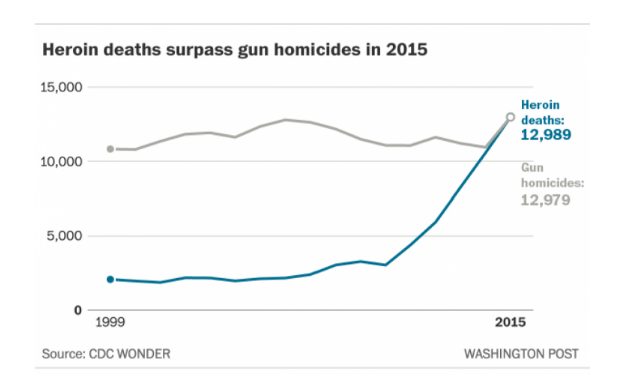
Heroin deaths just surpassed deaths by gunshot. Congratulations, opioid-shilling pharma companies!
Medicaid
For those looking for more insights into Medicaid, I highly recommend a few articles that provide perspective on post-election changes, hospital payments from Medicaid.
ACA repeal
Billy Wynne has a really thoughtful piece on why ACA will not be repealed. Certainly made me think differently about a few issues. FWIW, I’ve heard from a colleague who is Chair of a large health plan that the repeal language is already written.
These perspectives may both be right; I expect a re-branding of ACA and not a total repeal. The impact on the health system, hospital finances, the individual insurance market, and the number of insureds of a complete and sudden repeal would be disastrous.
Rather, the GOP will pass a bill ostensibly “repealing” ACA while in fact keeping many of its changes in place for at least three years.
How will Democrats handle this? Here’s one perspective.
Enjoy the weekend. Gonna get a load of snow up here in upstate New York – can’t wait.