Workers’ comp is singularly ill-equipped to handle COVID-19…but some organizations are making solid progress
The industry’s antipathy towards change, resistance to anything smacking of risk, and rejection of most anything remotely “innovative” ensures many payers, vendors, regulators and other stakeholders won’t be able to handle the fallout from COVID-19. Industry veterans know that any change is brutally hard, slow, and fulls of fits and starts; if there’s a business that struggles mightily to innovate its workers’ comp.
Few WC organizations will adapt quickly enough to keep pace. Executives get promoted for not making mistakes, for squeezing vendors, for cutting administrative expenses – not for innovating, taking risks, being creative. These “attributes” are exactly what organizations don’t need if they are to survive the next few months. Example – many payers are viewing COVID-19 thru the lens of yesteryear, acting as if the future will be the same as the past.
It won’t be.
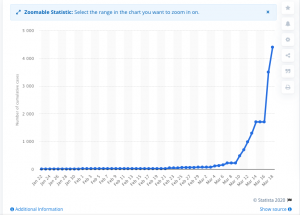
Covid-19 will change workers’ comp in ways that would have been incomprehensible just a week ago.
But some are moving quickly.
Two big insurers are suspending premium collection – a huge shout out to Chesapeake and BWC Ohio for leading the way. Kudos to the State Fund of California for suspending policy cancellations and penalties for late payments.
Others may follow…for good reason. Workers’ comp insurance has been very profitable of late and most insurers can afford to tap into cash reserves.
Tele-everything is exploding, albeit haphazardly. Regulators in many states are scrambling to enable/allow/legalize the use of telemedicine in its many forms. Vendors are struggling mightily to keep up with the patchwork of state-specific regulations which are different today than they were yesterday. Payers that pooh-poohed the very idea of telemedicine, or slow-walked it, or had programs in name only are beating down vendors’ doors, demanding access to a service they gave short shrift to just a week ago.
Inevitably, mistakes will be made – what was OK yesterday isn’t going to be tomorrow, and program requirements, procedures, approval processes, and forms are all in a state of flux. This is where the IAIABC could be hugely helpful; The IA is uniquely positioned to bring regulators together to agree on a standard set of guidelines and regulations that should be adopted by each state. These should be fast-tracked because telemedicine will be critical to ensuring injured workers get the care they need.
Regulators and industry executives that ponder, debate, discuss, and dither will do harm to patients, providers, and policyholders alike. Of course there will be things they won’t like or that “won’t fit” – but now is not the time to argue, it is the time for action.
This does NOT mean employers and insurers shouldn’t embrace telemedicine and telerehab, just make sure you are working with vendors experienced in the space. Concentra is one, MedRisk (HSA consulting client) is another. Carisk (also HSA consulting client) is able to deliver services to their cat/complex patients via their proprietary application. The company is also providing access to behavioral health services via telepsych.
For those in the Independent Medical Exam space, you may be able to ply your trade remotely. Register for Chris Brigham’s webinar Working in the Virtual World – Practical Steps for the MedicoLegal Expert here. It’s tomorrow, Wednesday March 25 at 3 pm eastern.

And for those of us in need of a refresher in coping skills – which includes pretty much all of us – register for David Vittoria’s terrific (and free) half-hour webinar Calm Amidst the Chaos: Taking Care of Ourselves & Others When Things are Stressful. Sign up here.