Obsessing over stuff we don’t know and can’t control will make us nuts.
Instead, focus on what you can do to protect yourself and your loved ones, and help others any and every way you can.
Why you should ignore a lot of the “experts” and their models.
Just two days ago I said: Ignore anyone who says we’ll be back to normal by this date or that.
I’ll add – Ignore anyone who says there will be this many infections and this many deaths – their “models” are based on data that is likely wildly inaccurate and make assumptions that differ wildly.
(the model used in White House press briefings assumes all states impose lockdowns similar to China’s and keep them in place for months. Meanwhile, the President is talking about a lockdown that ends in a few weeks and many states were late imposing lockdowns – or haven’t yet.)
A basic rule of statistical analysis is “when different studies of the same thing don’t agree it’s probably because they aren’t counting the same stuff the same way.” (OK, I sort of made that up – but it’s entirely true.)
A percentage is based on a numerator (the top number), which in this case is the number of people who died “of COVID”, divided by the denominator – the number of people “infected”.
First, the numerator – deaths due to COVID.
What?? How can this be? Is it because Italians are older? no…Germany’s population is older than Italy’s. Are Israelis healthier? Well…
From the BBC – “it might seem simple enough: if a patient dies while infected with Covid-19, they died of Covid-19.” Perhaps – but they may have died from a car accident, or might have an underlying health condition such as COPD or asthma or heart disease. The UK counts ANYONE who dies and has tested positive for COVID as a COVID death. Even if they died in a car accident.
Here in the US, physicians have discretion; they report whether the patient died “as a result of this illness.” So, it’s not surprising that the UK would have a higher death rate than the US.
A related issue – reports from Italy indicate there are a lot more people dying of all causes than usual, and many of those “extra” deaths aren’t attributed to COVID. “Only 12 per cent of death certificates have shown a direct causality from coronavirus,” said the scientific adviser to Italy’s minister of health last week. [source here]
So, we do not know the actual number of people who have died “as a result of COVID.”
Now, the denominator – the number of people “who have COVID.”
Different countries also report different “infection rates”;
- China may not report people who test positive but don’t show symptoms (are “asymptomatic”). As a substantial percentage of people who get infected don’t show symptoms, that makes China’s “infection rate” seem a lot lower than it really is.
- The number of tests isn’t as useful as the percentage of people tested. Reality is, if we aren’t testing everyone, we don’t know the real percentage of people with COVID.
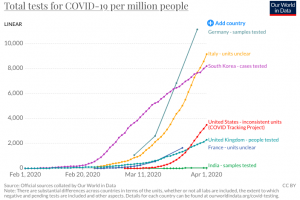
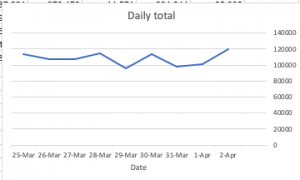
- Here in the US we are STILL way behind testing; we’re only testing about a hundred thousand people a day – about the same number we tested 9 days ago.
Oh, and there are two different “fatality rates.”
Again the BBC:
There are, in fact, two kinds of fatality rate. The first is the proportion of people who die who have tested positive for the disease. This is called the “case fatality rate”. The second kind is the proportion of people who die after having the infection overall; as many of these will never be picked up, this figure has to be an estimate. This is the “infection fatality rate”.
Head swimming yet? Yeah, mine too. Net is no one knows how many of us are infected and we don’t know the number of people who die of COVID-related conditions.
We DO KNOW:
- social isolation will help keep you safe;
- sanitizing everything will help keep you safe;
- helping others will help keep you sane.
What does this mean for you?
Obsessing over stuff we a) don’t know and b) can’t control will just make you nuts. Focus on what you can control.
And be nice.

We have suddenly entered a crisis of uncertainty which erodes trust. the workers’ comp field needs its leaders to assure employers and workers that the disruptions to claiming, medical recovery and RTW are being to be quickly understood and whatever adjustments that need to be made will be made without delay. Trust at this time is a rare and extremely valuable commodity. Joe, you are stepping up to the challenge.
thanks Peter. Much appreciate it.
Great post. It is very important that we keep our wits about us. Everyone needs to make sure they are checking and double-checking the source of any information you are receiving. It was bad before this; it’s worse now. I have received everything from well-intended misinformation to outright BS from people who should know better. Facts are more important now than ever and because we still know so little, we want to accept as fact whatever we hear. As your posts consistently point out, that is a very dangerous road to take. Wishing peace and health to all.
Thanks Fred – have an excellent weekend
We are not going to “test” our way out of this pandemic. A COVID-19 test will only provide with some level of certainty (unsure sensitivity/specificity of the various tests) the status of an active infection at a single point of time. With shelter-in-place orders in most all heavily infected areas, a positive test does not change next steps/care in most scenarios. We should be thinking about the appropriate utilization of “testing” and it should be limited to those scenarios where a positive test will change how a patient is treated clinically or actions the patient should take.
The negative consequence of the media continuing to run with the “we are not doing enough tests” headlines/stories is individuals are seeking out testing in scenarios where a positive test would not change clinical care or actions. These additional unnecessary tests result in slower processing of actual tests where clinical care or actions would change. These unnecessary tests also result in additional strain on PPE (masks/gloves/etc.) and collection materials (swabs, etc.). In scenarios where individuals are seeking out tests and they are then denied testing due to not meeting qualifications, they have just exposed themselves and likely their family and others by leaving their house and visiting an area where other potentially infected individuals are.
This pandemic is not going to end until either enough people get infected, recover, and have immunity (herd immunity), a vaccine is developed and enough people are inoculated (herd immunity), or meaningful treatment is discovered (drastically reduces mortality rate among infected). Until then, those of us who have not yet gotten COVID-19 need to protect ourselves from becoming infected.
Hello Scott – thanks for the comment re testing. Agree, there are many dimensions to this.
One other thought – testing everyone would be best as it appears many who have COVID are asymptomatic, and if one knows they are infected they can take additional precautions. Unfortunately despite statements to the contrary the US is way behind other countries due to a series of missteps. Hopefully that will be corrected quickly
Even if there were an unlimited number of tests and healthcare resources to test everyone, I think testing everyone would cause more issues than it would solve. The test is by not 100%, there are false positives and false negatives, it also only good for a single point of time, and TAT is not immediate. A negative test today could turn positive tomorrow after the individual went to the testing site and encountered infected individuals. Almost all areas of high infection are under shelter-in-place orders. Unless you are an individual that needs significant clinical care/hospitalization a positive or negative test does not change what you should be doing. Asymptomatic individuals should be “sheltering in place” regardless of if they were tested or not. A negative test should not be thought of as a hall pass to congregate in public.
I do not believe the US is “way behind other countries”. The US is much larger and much more diverse than almost all of the other countries with high infection rates that are reporting (China being the larger but less diverse). Germany, Italy, South Korea, UK, etc., all have geographic foot prints and populations smaller or not much bigger than some of our states. Our resource allocation and healthcare strategy is going to look different in the various states, NY is not MT, TX is not CA, FL is not ME, etc. Even within States, urban and rural areas have different strategies and challenges.
Hi Scott – thanks for the thoughtful response; appreciate your perspective.
I don’t understand why testing everyone would be problematic as it would solve the second biggest problem we have today – transmission by those who do not know they are infected. There are 45 minute tests in final development stages today which can be delivered in physician office and clinic settings; this will greatly ramp up our ability to test.
All the data I’ve seen shows the US is far behind other countries in testing. Previous posts – and this one – show data that indicates the US is far behind other countries on testing per capita. Perhaps I’m missing something here, but I don’t see what diversity of population has to do with this; if it does, China is MUCH more diverse than the US as there are literally hundreds of different groups among the 1.3 billion residents. Europe is also much more diverse than it was historically – but again, I don’t see how that bears on this. If I’m missing something happy to know what it is.
Sure, I will try to explain my line of thinking. Knowing if you are asymptomatically carrying or not, should not change what you should be doing in 80%+ of cases (healthcare workers or essential workers are exceptions). Almost all infected areas are under shelter-in-place restrictions. Therefore if you are infected or not, you should not be mingling with others outside of your household.
Testing per capita. These metrics look at the US as a country and not the geographical locations that are more comparable to the other comparable countries. Significant areas of the US do not have the need to do as widespread testing/evaluation as others but are included in the denominator of “per capita”. A “per capita” number of just NYC or NY should be magnitudes higher than a “per capita” number of the US.
Diverse may have not been the best word, to describe the drastic and dramatic differences in lifestyles and habits across our country. In this aspect, I believe the US is much more diverse than the countries being compared to. We have parts of our country still in deep snow and other parts of our country sun tanning on the beach. We have parts of our country who live in very urban areas and large parts of our country that live in extremely rural areas, their daily activities and interactions with people are significantly different. There are certainly cultural habits that have both contributed and decreased COVID-19 transmission and spread, but that is another topic.
China is definitely an outlier in all of this as very little information coming out of that country is trustworthy (IMO). China’s governmental structure also allows them to respond drastically different than the US (at the cost of liberties we enjoy here).
Hey Scott – I really appreciate your thoughtful and detailed comment.
I agree that all of us should be doing the right thing; alas many aren’t. There’s just a lot of knuckleheads out there (like I was 40 years ago) who might be smarter if they knew they were carrying the virus…Even more troubling, states aren’t all doing smart stuff: Florida finally instituted a shelter-in-place order, except it doesn’t include churches, for reasons that escape logic.
testing per capita – Agreed – testing should be preferentially done in areas where there appear to be more cases. That said, what scares me about this virus is it could well be that coronavirus has spread much deeper and farther than anyone suspects. Without testing we just don’t know – and knowledge would be really helpful in planning and preparing.
Not sure we are on the same page re other countries. Northern Japan is like Alaska; Okinawa is like Ha’waii. China has everything from jungles to high mountains, Uighers to Tibetans to Mongols to Szechuanese; perhaps we’ll just agree we see it differently. I do agree that Chinese data is suspect.
be well – Joe
Great piece, Joe. I can’t wait to read the post-mortem in a year or so. Will this be remembered as the greatest threat mankind has ever faced or a massive overreaction to a manageable problem? Hopefully, we’ll all be around to find out.
Hi Mike
Hope you and the family are thriving on the Neck.
My guess – and it is just that, a guess – is this will be somewhere between those two endpoints, but more towards the disaster end. What’s apparent is the real death toll is grossly undercounted; the. Reporting from Bergamo Italy reflects a much higher toll than the official data. While covid won’t kill on the scale of the Black Death or Ebola, it is currently killing about 2.7% of those diagnosed in the US.
The impact on the economy, our healthcare system, and are standing in the world will have deep and far-reaching consequences. One only needs to compare our infection rate to every other country, The feckless response of our elected leaders, and the pending collapse of our healthcare system to see our leadership position in the world is fading fast.