In Maryland and Hawai’i, docs are claiming that they pay much more for drugs than retail pharmacies, therefore they are justified in getting paid a lot more than retail pharmacies.
Bullshit.
Now that I’ve got your attention, here’s the truth.
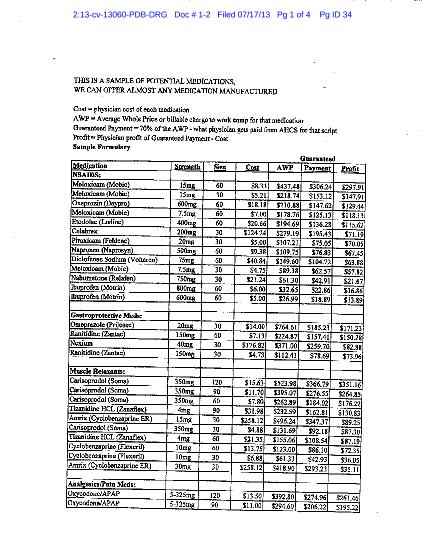
This is just one page from a document was included in All State v Prescription Partners, a lawsuit filed by the big insurer in Federal court last summer. It is described as “the drug list included in the “sales pitch” of AHCS…”
It is pretty much self-explanatory.
What does this mean for you?
Two things.
1. Legislators should demand proof from dispensing advocates that their costs are higher and justify their outrageous prices.
Clearly they are not, and dispensing advocates testifying that their costs justify their prices are misleading/uninformed/duplicitous.
2. More evidence of the ongoing effort by profiteers looking to suck money out of employers and taxpayers.

{kind=link}
Joe:
But how do you really feel about these docs. Such language and so early in the morning! Well said!
Any facts on why the cost of Hydrocodone, Oxy, Vicodine and Morphine has skyrocketed over the last 6 months?
Is this a strategy to deter prescribing? the result of some adverse effect in the manufacturing world? or another exercise in profiteering?
45 days ago – a prescription for 12 tablets 5-325 at CVS ran $26.64…and the prices have gone up since then. Folks in Big Pharma have said 95% of all Vicodin/Oxy/Hydrocodone are sold in the US – is that a fact?
Why is it legal for a Doc to dispense meds from his office. I am a “lay” person but I thought you needed a pharmacist license to dispense medications, especially narcotics. If you have a Pharmacist in your Urgent Care clinic, I think you can not only justify it but it mitigates the legal ramifications. But an Occ Med Mill?
Some of these injured workers have never taken meds before and believe the US provides the best medical care in the world.
They walk out with bags of narcotics, muscle relaxers, anti-inflammatories, Soma, Fentanyl, Flexeril, Oxy…they could die from an overdose.
Risk vs Reward…when it is patient risk vs Doc reward…prescription for disaster. When carriers pay for these narcotics during treatment and then include them in FMTA, I think there is a real foundation for the fact the carriers has become the “pusher man” and is the “deep pocket” when a patient becomes and addict, overdoses and dies.
These FMTA for narcotics only are so unsupervised we have no way of knowing if those drugs are a revenue source for the latest addict or that we are under-writing their newest business venture – being a pusher.
If CVS is charging $2 a tablet, what is the street price? And we dispense in lots of 180 – 240 per prescription. That is a lot of financial gain. Do we even require a simple, cheap drug test to demonstrate the patient is taking the medication appropriately? Carriers need to wake up and protect themselves, their clients and the public.
Like I said, I am a lay person…a Grandma. How many babies pick up a pill off the floor or find it in the couch? Prescription for tremendous grief, pain and loss.
What does it Pfizer pay for the ingredients in Celebrex?